Background Context
Per a News Release in September 2022 (link below), “More than 30 million Americans have T2D, but despite the availability of many medications to treat diabetes, only around half of US adults with T2D achieve target haemoglobin A1c (HbA1c; a measure of blood sugar control) of less than 7% [2]. Higher HbA1c levels are associated with complications like heart disease, stroke, kidney disease (nephropathy), eye disease (retinopathy) and nerve disease (neuropathy).” Diabetes patients taking Mounjaro (chemical name: Tirzepatide) reached the standard T2D treatment goal of under-7 A1C faster than other traditional diabetes drugs. Unlike Insulin, it conveys weight loss instead of weight gain and reverses insulin resistance (whereas the administration of insulin increases insulin resistance). ADA recommends GLP-1RA drugs prior to insulin as first step for injection therapy naive T2D patients failing to reach under-7 A1C goal using traditional therapies.
Latest type 2 diabetes drug achieves blood sugar and weight targets faster
https://www.eurekalert.org/news-releases/964588
Mounjaro is the brand name for the molecule Tirzepatide, created by Eli Lilly. It is part of the class of drugs that activate at least one of the body’s digestive (incretin) hormone receptors to initiate optimal metabolic handling of food eaten. This class of drugs or therapeutic approach was pursued because research showed that the endocrine system of diabetics have dysregulations in the body’s handling of food eaten. Molecules in this class of drugs are referred to as incretin mimetics: they mimic the behavior of hormones that work more optimally in non-diabetic people’s metabolisms.
Specifically, drugs in this class have some or all of the following features in common:
Drugs in this class are typically delivered via injections at routine intervals, and are frequently available in multiple doses for various strengths, based on the patients’ needs, results and tolerance. Prior to Mounjaro, they were referred to as “GLP-1 analogues,” (GLP-1 stands for glucagon-like peptide 1). In peer-reviewed journal articles, these are sometimes referred to as “GLP-1RA drugs” (RA stands for Receptor Agonist). One downside of these GLP-1 drugs has been the frequency of gastrointestinal adverse events or side effects, in particular, nausea, vomiting or diarrhea. While these GI-related side effects are not life-threatening, one who experiences these side effects is less likely to continue the drug and successfully achieve therapeutic benefits.
Examples of other drugs in this class that pre-date Mounjaro:
Brand Name Molecule Name Prescribed on-label for Injection Timing
Ozempic Semaglutide Type 2 Diabetes Weekly
WeGovy Semaglutide Weight Loss Weekly
Trulicity Dulaglutide Type 2 Diabetes Weekly
Byetta Exenatide Type 2 Diabetes Weekly
Victoza Liraglutide Type 2 Diabetes Daily
Saxenda Liraglutide Weight Loss Daily
Why’s Mounjaro a Big Deal?
Mounjaro is the first dual-receptor agonist drug to hit the market. Dual-receptor means that instead of only acting on the GLP-1 hormone receptor, it also acts on a second incretin hormone receptor, the GIP hormone receptor. Combined activation of both receptors was found to act synergistically, providing additive effects, enhancing glucose control and weight loss compared to just GLP-1 analogues alone.
In trial studies, Mounjaro (tirzepatide)’s effectiveness exceeded all prior-generation medications and also insulin, for reducing A1C, reducing triglycerides, and weight reduction, including intra-abdominal fat and liver fat. The results were significantly greater than last generation medications, both in results and time to achieve results. Trial participants remarked that exercising caloric restriction, which usually is an obstacle to weight loss and results in increased hunger, instead came easily, and the GI-related side effect of nausea is reduced due to the GIP-RA being activated. Research was done to investigate use of Mounjaro as an add-on to other treatments such as metformin and insulin, but also to investigate its use as a monotherapy, which would enable patients to drop other medications altogether. Weight loss results are similar to bariatric surgery, but unlike bariatric surgery, Mounjaro doesn’t generate increased hunger long-term due to the reduced absorption of calories.
Mechanisms underlying tirzepatide efficacy revealed
Medicine Matters, 4/28/2022
Tirzepatide, a New Era of Dual-Targeted Treatment for Diabetes and Obesity: A Mini-Review
Molecules, July 2022
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9268041/
Tirzepatide, a dual GIP/GLP-1 receptor co-agonist for the treatment of type 2 diabetes with unmatched effectiveness regrading glycaemic control and body weight reduction
Cardiovasc Diabetol. 2022 Sep
https://pubmed.ncbi.nlm.nih.gov/36050763/
Tirzepatide generated extra weight loss compared to semaglutide and they are not sure why, as both drugs decreased appetite and food intake equally. Data on the results from one study are below. It’s believed that the coadministration of an agonist fit GLP-1 and GIP receptors gives greater results than the administration of one alone.
“At 28 weeks, reductions in body weight from baseline were observed with TZP 15 mg (-11.2 kg) and SEMA 1 mg (-6.9 kg) , and significantly differed between treatment groups (-4.3 kg [95% confidence interval [CI]: -6.8, -1.9]; p<0.001) . Reductions in fat mass from baseline were also observed with TZP 15 mg (-9.7 kg) and SEMA 1 mg (-5.9 kg) , and significantly differed between treatment groups (-3.8 kg [95% CI: -6.2, -1.4]; p=0.002) . Energy intake reductions from baseline observed with TZP 15 mg (-348.4 kcal) and SEMA 1 mg (-284.1 kcal) did not differ between treatment groups (-64.3 kcal [95% CI: -160.3, 31.7]; p=0.187) . TZP reduced overall appetite by increasing satiety with decreased PFC (all p<0.05) . Appetite ratings did not differ between TZP and SEMA. In conclusion, TZP achieved greater weight loss than selective GLP-1 RA, mostly driven by fat mass loss. Significant and clinically meaningful reductions in appetite and energy intake were observed with both TZP and selective GLP-1 RA. However, these effects could not totally explain the additional weight loss with TZP. As appetite and energy intake reduction were not significantly different between treatments; additional mechanisms might contribute to the weight loss with TZP. Ongoing studies will further elucidate the mechanism of weight loss with TZP.”
Tirzepatide Reduces Appetite, Energy Intake, and Fat Mass in People with T2D
Diabetes, June 2022
“Both GLP-1 and GIP are classified as incretins and are expressed throughout the body, including pancreatic beta cells and the gastrointestinal tract. These stimulate insulin secretion in a glucose-dependent manner.
Incretins are a group of metabolic hormones that are released from the enteroendocrine cells into the bloodstream after eating and stimulate a decrease in blood glucose levels. There are 2 incretins produced: GIP and GLP-1.
GLP-1 and GIP increase insulin from beta cells and glucose uptake by muscles and decrease blood glucose. GLP-1 stimulates glucose dependent decrease of glucagon from alpha cells, lowering glucose production from the liver and decreasing blood glucose.
GIP promotes the growth and survival of the pancreatic beta cell and stimulation of adipogenesis. Dipeptidyl peptidase-4 (DPP-4) is a serine protease responsible for the inactivation of GLP-1 and GIP. In patients with type 2 diabetes, there is decreased GLP-1 and GIP production.3
Tirzepatide’s protein sequence was based on the sequence of endogenous GIP and its pharmacological action on GLP-1 receptors is comparable to endogenous GIP. It is a 39 amino acid linear synthetic peptide conjugated to a C20 fatty diacid moiety.
The drug is also highly bound to albumin in the plasma, which prolongs its half-life.4 The long half-life of tirzepatide allows for a once-weekly dosing via subcutaneous administration. It is available in 6 doses: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, 15 mg.1
The mechanisms of action for tirzepatide include stimulation of first- and second-phase insulin secretion, as well reduced glucagon levels, both in a glucose-dependent manner. The drug delays gastric emptying, lowers fasting and postprandial glucose concentration, decreases food intake, and reduces body weight in patients with type 2 diabetes. In addition, tirzepatide increases insulin sensitivity.
The glycemic and weight control effects of this drug are believed to arise from dual agonism at GIP and GLP-1R. Studies have demonstrated that coadministration of a GIP and GLP-1R agonist significantly increases insulin response and suppresses glucagon secretion compared to separate administration of either hormone alone.2
In clinical trials, tirzepatide was compared to semaglutide (GLP-1), insulin glargine and insulin degludec. Participants in the SURPASS-2 program achieved better average hemoglobin A1C reductions with tirzepatide than semaglutide.4
In the SURPASS-3 program, tirzepatide was superior to titrated insulin degludec, with greater reductions in HbA1c and body weight at week 52 and a lower risk of hypoglycemia.5 SURPASS-4 study evaluated patients with type 2 diabetes and elevated cardiovascular risk. Compared with glargine, tirzepatide demonstrated a greater and clinically meaningful HbA1c reduction with a lower incidence of hypoglycemia at week 52. Tirzepatide treatment was not associated with excess cardiovascular risk.”
Clinical Overview: Tirzepatide for Type 2 Diabetes
Pharmacy Times, September 2022
https://www.pharmacytimes.com/view/clinical-overview-tirzepatide-for-type-2-diabetes
Mounjaro’s Relevance to Diabetes
Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial
The Lancet, June 2021
https://pubmed.ncbi.nlm.nih.gov/34186022/
Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomised, open-label, parallel-group, phase 3 trial
The Lancet, August 2021
https://pubmed.ncbi.nlm.nih.gov/34370970/
Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial
The Lancet, April 2022 (paywall)
https://www.thelancet.com/journals/landia/article/PIIS2213-8587(22)00070-5/fulltext
Efficacy of once-weekly tirzepatide versus once-daily insulin degludec on glycaemic control measured by continuous glucose monitoring in adults with type 2 diabetes (SURPASS-3 CGM): a substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial
The Lancet, April 2022 (paywall)
https://www.thelancet.com/journals/landia/article/PIIS2213-8587(22)00077-8/fulltext
Effect of Subcutaneous Tirzepatide vs Placebo Added to Titrated Insulin Glargine on Glycemic Control in Patients With Type 2 Diabetes: The SURPASS-5 Randomized Clinical Trial
JAMA, February 2022
https://pubmed.ncbi.nlm.nih.gov/35133415/
Mounjaro’s Relevance to Weight Loss
Goal for weight loss medications is to reach an endpoint of 5% weight loss. In the SURMOUNT-1 trial, there were 2,539 participants. Tirzepatide trial participants lost 20.9% of overall body weight in 72 weeks. About a third of people on the highest two tirzepatide doses lost at least a quarter of their bodyweight during 72 weeks of treatment. All participants received regular lifestyle counseling over the course of the trial, promoting healthy, balanced meals, a 500 calorie per day deficit, and 150 recommended minutes of exercise per week, but the placebo group only lost an average of 3.1% of their bodyweight.
Can New Weight-Loss Drugs Really Treat Obesity?
Yale Medicine, June 2022
https://www.yalemedicine.org/news/new-medications-treat-obesity
“GLP-1 is of relevance to appetite and weight maintenance because it has actions on the gastrointestinal tract as well as the direct regulation of appetite. It delays gastric emptying and gut motility in humans. In addition, interventricular injections of GLP-1 inhibit food intake, independent of the presence of food in the stomach or gastric emptying. Peripherally administered GLP-1 also affects the central regulation of feeding. It is therefore the synergistic actions of GLP-1 in the gut and brain, acting on both central and peripheral receptors that seem responsible for the effects of the hormone on satiety.
…unlike pure dietary measures, weight loss may be sustained for up to a period of 3 years in the presence of GLP-1 agonist therapy [67, 68]. However, once therapy is discontinued, there is some regain of weight [69]. There seems to be minimal effect of GLP-1 on energy expenditure per se and thus the overall negative energy balance seen with GLP-1 therapy is largely a result of decreased energy intake [70].”
Effects of GLP-1 on appetite and weight
Reviews in Endocrine and Metabolic Disorders, 2014
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4119845/
Below, some info about how semaglutide works (which is a GLP-1RA drug that was released before Mounjaro under the brand names Ozempic & WeGovy):
How a lizard’s venom inspired the promising weight loss drug Wegovy
Vox, July 2021
https://www.vox.com/22553793/gila-monster-lizard-venom-inspired-obesity-drug-semaglutide
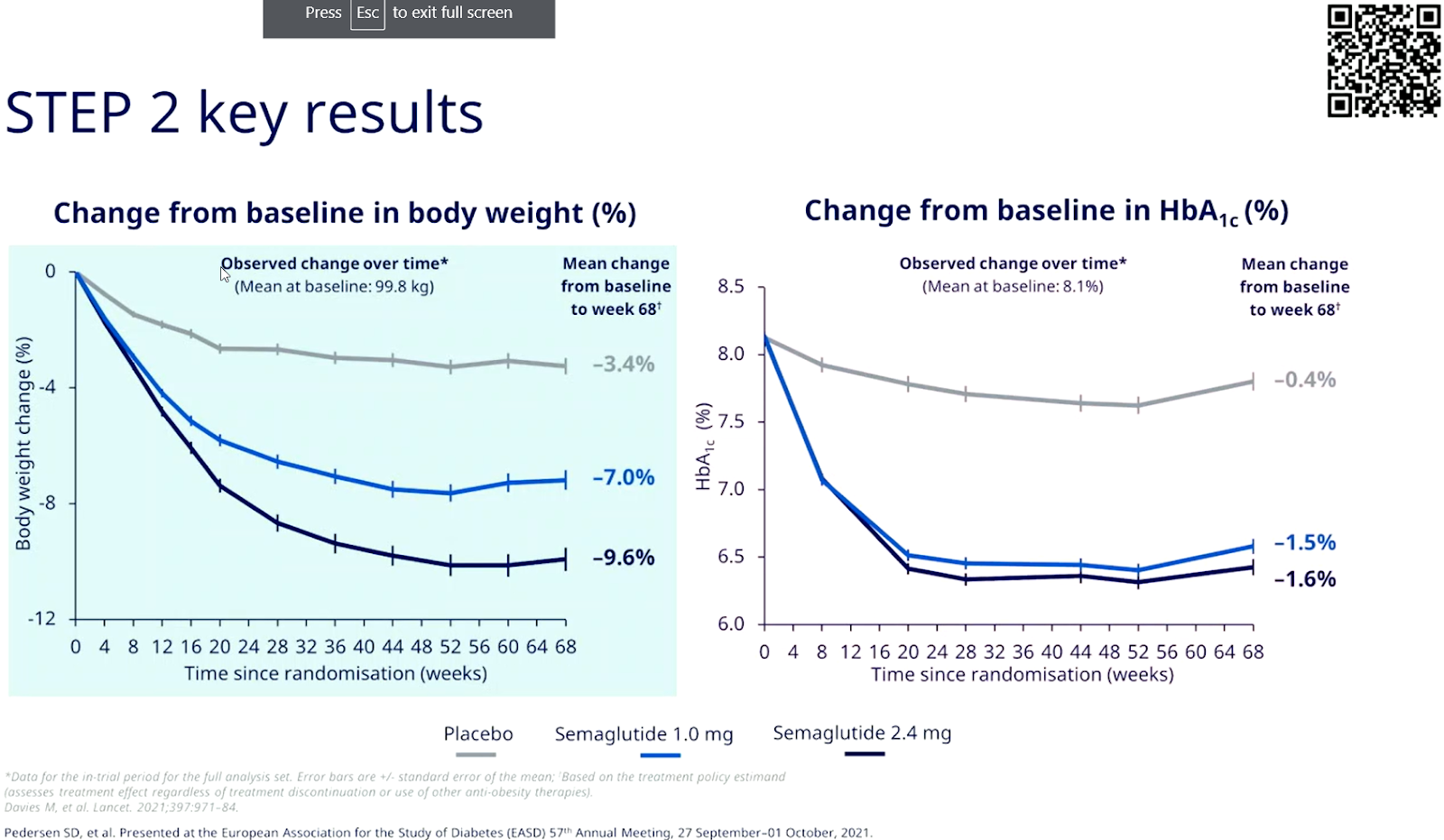
Below is a screencap and a link to a video presentation of key results from a STEP 2 Trial on Ozempic, where they did research for 68 weeks on 2.4mg of Semaglutide (Ozempic/WeGovy) on T2D weight loss.They saw more vomiting at 2.4mg (20% vs 13% vomiting at the 1mg). Most of the A1C benefits are reached with Ozempic at 1mg, and the difference at higher doses is seen in weight loss. There are links to other video presentations about Tirzepatide (Mounjaro) results in the SURPASS-2 and SURPASS-5 trials as well on this page.
Effect of semaglutide 2.4 on glucose metabolism and body weight in adults with overweight or obesity and type 2 diabetes in the STEP 2 trial
https://www.easd.org/media-centre/home.html#!resources/b-effect-of-semaglutide-2-4-mg-on-glucose-metabolism-and-body-weight-in-adults-with-overweight-or-obesity-and-type-2-diabetes-in-the-step-2-trial-b
Mounjaro’s Relevance to other conditions (Heart Disease, Liver, Kidneys, Nervous System, Learning & Memory Abilities, Body Fat, Insulin Resistance, Bone Density, Metabolism, Inflammation & Inflammatory Disorders, Osteoarthritis)
Gastrointestinal Incretins – Glucose-Dependent Insulinotropic Polypeptide (GIP) and Glucagon-like Peptide-1 (GLP-1) beyond Pleiotropic Physiological Effects Are Involved in Pathophysiology of Atherosclerosis and Coronary Artery Disease – State of the Art
February 2022, Biology
https://www.mdpi.com/2079-7737/11/2/288/htm
Mayo Clinic “Expert Answers” explanation
https://www.mayoclinic.org/diseases-conditions/type-2-diabetes/expert-answers/byetta/faq-20057955
Mounjaro: Its Powerful Potential to Treat Diabetes & Obesity
Coverage of the ADA Scientific Sessions – Beyond Type 1 & the ADA
https://beyondtype1.org/mounjaro-results-obesity-type-2-diabetes/
Press Release: Latest Data from SURPASS Trials Demonstrate Tirzepatide Provided Meaningful Blood Sugar Reductions
June 29, 2021 – American Diabetes Association
SURMOUNT-1 places tirzepatide weight loss efficacy within surgical range
June 4, 2022 – Medicine Matters diabetes
https://diabetes.medicinematters.com/ada-2022/tirzepatide/surmount-1-weight-loss-efficacy/23127764
A Quick Guide to the SURPASS and SURMOUNT trials, Phase 3 trials of Tirzepatide in Type 2 Diabetes and Obesity.
(This article also contains links to quick guides to ALL the GLP-1 trials, plus lists what current trials are ongoing and their estimated study completion dates)
Updated August 2022 – Medicine Matters diabetes
Tirzepatide Once Weekly for the Treatment of Obesity
July 21, 2022 – New England Journal of Medicine
https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
Do I have to have Diabetes to take Mounjaro?
No. Many prescriptions are able to be written for off-label reasons, as this practice is very common, however your success with acquiring this prescription may vary. This is depending on your physician’s comfort with this practice, or even their organization’s policies which might forbid those in their practice from doing so. You’ll need to check with them and perhaps look around for recommended providers if you don’t feel comfortable with the answers you get.
Recent Advances in Incretin-Based Pharmacotherapies for the Treatment of Obesity and Diabetes
March 2022
https://www.frontiersin.org/articles/10.3389/fendo.2022.838410/full
The Role of GLP-1 in the Metabolic Success of Bariatric Surgery
Endocrinology, December 2017
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5711387/
Bodyweight rebounds after semaglutide withdrawal
Medicine Matters 5/9/2022