Research · Single-study breakdown
What the mazdutide obesity trial (GLORY-2) actually showed
What this means for you
If you carry extra weight — whether or not you have type 2 diabetes — this is an early read on a drug that may eventually widen the weight-and-metabolism toolkit. Obesity and type 2 diabetes sit on the same metabolic spectrum, and taking off this much weight tends to pull blood pressure, triglycerides, and cholesterol in a healthier direction too, which is what this trial found.
A few honest caveats matter here. Mazdutide is not FDA-approved in the United States. The trial was run entirely in China, where lower doses are already approved; the 9 mg dose tested here is the higher end of the range. So this is not something you can ask for at a US pharmacy today. And the stomach side effects were common enough to take seriously, even though few people quit over them.
None of this is a reason to change what you are doing now. It is a reason to understand where obesity and diabetes treatment is heading, and to ask your doctor what is actually available to you.
How the trial was run
GLORY-2 was a phase 3, double-blind, placebo-controlled, randomized trial run at 27 hospitals in China between December 2023 and November 2025. It enrolled adults with obesity — a body mass index of 30 or higher — and randomized 462 of them in a 2:1 ratio to once-weekly subcutaneous mazdutide or placebo, both added on top of a reduced-calorie diet and increased physical activity. Mazdutide was not started at its full dose: it began at 3 mg once weekly and was raised by 3 mg every four weeks until it reached the 9 mg maintenance dose. The treatment period lasted 60 weeks. The trial was funded by Innovent Biologics, which develops mazdutide in China under license from Eli Lilly.
The participants were younger and earlier in their disease than in many Western obesity trials: mean age 33.9 years, 64% women, mean body weight 94 kg, and mean BMI 34.3. About one in six — 16.1% — also had type 2 diabetes, and 86.6% had at least one weight-related health problem, so this was predominantly, but not only, a non-diabetic obesity population. Retention was high: roughly 90% of the mazdutide group and 95% of the placebo group completed treatment.
What the data showed
The two co-primary endpoints were the percentage change in body weight at week 60 and the proportion of people who lost at least 5% of their weight. Mazdutide cleared both. Average body weight fell 16.65% on mazdutide versus 1.50% on placebo — a placebo-adjusted difference of about 15 percentage points (95% CI, −17.22 to −13.09; P < .001), or roughly 15 kg in absolute terms. And 84.3% of the mazdutide group lost at least 5% of their body weight, versus 33.1% on placebo.
The deeper the cut, the wider the gap. The proportion reaching at least 10% weight loss was 69.9% on mazdutide versus 14.4% on placebo; at least 15%, 57.3% versus 6.5%; and at least 20%, 42.4% versus 2.6%. In other words, more than half the people on mazdutide lost at least 15% of their body weight, a threshold few reached on placebo.
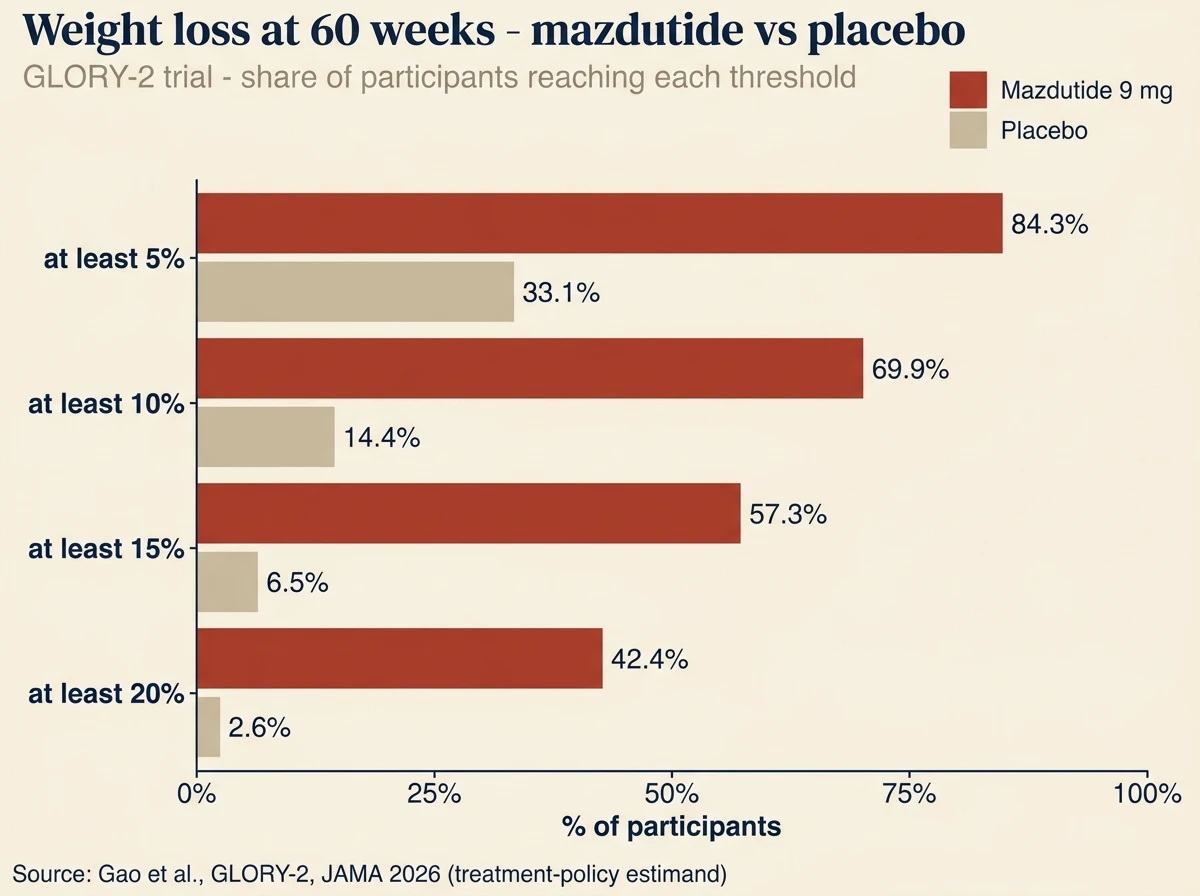
Share of participants reaching each weight-loss threshold at week 60 (treatment-policy estimand). Source: GLORY-2, JAMA 2026.
Weight wasn’t the only thing that moved. The trial tracked a panel of cardiometabolic measures as key secondary endpoints, and mazdutide beat placebo on all of them: waist circumference fell about 13 cm (versus 2 cm), systolic blood pressure dropped nearly 10 mm Hg, and triglycerides, non-HDL cholesterol, and LDL cholesterol all declined. This is the pattern you would expect when a drug removes this much weight, and it is part of why obesity and type 2 diabetes are treated as facets of one underlying metabolic problem rather than separate conditions.
The cost showed up in tolerability. Gastrointestinal side effects were common and far more frequent than on placebo: vomiting occurred in 53.1% of the mazdutide group versus 1.3% on placebo, nausea in 46.9% versus 3.2%, and diarrhea in 39.4% versus 6.5%. Most of these events were mild to moderate and clustered during the dose-escalation phase, and the rate of serious adverse events was only modestly higher than placebo (7.2% versus 5.2%). Critically, only 2.9% of the mazdutide group stopped treatment because of side effects, and none did on placebo. The stomach effects were widespread but, for most people, not bad enough to quit over.
How mazdutide is different: the glucagon angle
Most of the weight-loss medicines in the headlines act on a single gut hormone, GLP-1. Semaglutide — Ozempic and Wegovy — is a GLP-1 receptor agonist. Mazdutide is a dual agonist: it activates the GLP-1 receptor and the glucagon receptor at once. It is a synthetic analog of oxyntomodulin, a natural hormone that hits both targets.
The GLP-1 side does the familiar work — blunting appetite and slowing stomach emptying so people eat less. The glucagon side is the twist. Glucagon is best known for raising blood sugar, which sounds like the wrong direction for a metabolic drug, but glucagon-receptor activation is also thought to increase energy expenditure and to act on the liver. The idea behind dual agonists is that combining the two adds weight loss and metabolic benefit beyond GLP-1 alone — and in the subgroup that was imaged, mazdutide cut liver fat substantially. GLORY-2 wasn’t designed to isolate how much the glucagon arm contributed, but it is the reason mazdutide is treated as its own class rather than another GLP-1.
Mazdutide vs the GLP-1 drugs you’ve heard of
It is tempting to line mazdutide up against tirzepatide (Mounjaro, Zepbound), semaglutide, and the new oral GLP-1 orforglipron and rank them by weight loss. Resist that. None of these have been tested head-to-head against mazdutide, and weight-loss numbers from separate trials — different countries, populations, and lengths — are not directly comparable. GLORY-2’s participants, for example, were notably younger and enrolled entirely in China, where people tend to develop weight-related complications at a lower BMI.
What does compare cleanly is design. Mazdutide is a once-weekly injection acting on GLP-1 and glucagon. Tirzepatide is also a weekly injection, but its second target is GIP, not glucagon. Semaglutide is a weekly injection (with an oral version) acting on GLP-1 alone. Orforglipron is a once-daily pill acting on GLP-1 alone — the same class as semaglutide, but with no needle. Different hormone combinations, different delivery, and — as GLORY-2’s side-effect numbers show — different tolerability trade-offs. The editorial published alongside the trial noted that mazdutide’s 53% vomiting rate ran higher than what is typically seen with GLP-1-only drugs, and closer to another glucagon/GLP-1 dual agonist.
When will mazdutide be available?
For now, mazdutide is largely a China story. Lower doses — 2, 4, and 6 mg — were approved in China in mid-2025 for long-term weight management, and later in 2025 for type 2 diabetes. The 9 mg dose studied in GLORY-2 is the higher end of that range, aimed at people with more severe obesity. In the United States, mazdutide is not FDA-approved, and GLORY-2 — a single trial conducted entirely in China — is trial evidence, not a US regulatory filing. Anyone outside China is watching the pipeline, not filling a prescription.
What this study can't tell us
- Run entirely in China — a single-country trial in a relatively young population (mean age 33.9); how well the results carry to other groups is not established here.
- 60 weeks — durability and long-term safety beyond about 14 months are unknown, and weight tends to return after stopping incretin drugs.
- No head-to-head versus semaglutide, tirzepatide, or other agents, so mazdutide cannot be ranked against them on this evidence.
- A heavy GI burden — vomiting, nausea, and diarrhea were common; real-world tolerability and adherence may differ from a monitored trial.
- Mostly a weight, not diabetes, trial — only 16.1% had type 2 diabetes, and weight loss was smaller in that subgroup, so this is primarily a weight-loss readout.
- Industry-funded — sponsored by Innovent Biologics, which had a role in the trial’s design, analysis, and reporting, as is common for phase 3 drug trials.
The number that will travel is the weight loss, and 16.65% over 60 weeks is a genuinely large effect for an obesity drug — with more than four in ten participants losing at least a fifth of their body weight. But the more useful read is what mazdutide represents: a second mechanism. After a decade in which GLP-1 was effectively the whole story, agents that add a glucagon or GIP signal are turning weight loss into a family of approaches rather than one drug repeated — and more mechanisms mean more options for the many people who don’t respond to, or can’t tolerate, any single one.
The honest counterweight sits right next to the efficacy. Side effects this common aren’t a footnote; they shape who will actually stay on a drug, even when few formally quit, and they were notably heavier here than with GLP-1-only medicines. And the geography matters: this is, for now, a Chinese approval-and-pipeline story, not a US one. For readers living on the obesity–diabetes continuum, mazdutide is worth knowing as a marker of where treatment is heading — not as something to act on today.
Frequently asked questions
1.Is mazdutide a pill or an injection?
Mazdutide is a once-weekly injection given under the skin. The once-daily pill in the same wave of news is a different drug, orforglipron.
2.Is mazdutide FDA-approved?
No. Mazdutide is not approved by the US FDA. It is approved in China — lower doses for weight management and for type 2 diabetes — and the 9 mg dose tested in GLORY-2 was studied for more severe obesity. The trial was run entirely in China.
3.How is mazdutide different from Ozempic or Mounjaro?
Ozempic (semaglutide) acts on one hormone receptor, GLP-1. Mounjaro (tirzepatide) acts on two, GLP-1 and GIP. Mazdutide also acts on two, but its second target is the glucagon receptor — a different combination, which is why it is considered its own class.
4.How much weight did people lose on mazdutide in GLORY-2?
On average, 16.65% of body weight at 60 weeks, versus 1.50% on placebo — about 15 kg. Roughly 84% lost at least 5% of their weight, and 42% lost at least 20%.
5.What are the side effects of mazdutide?
The most common were gastrointestinal. In GLORY-2, vomiting (about 53%), nausea (about 47%), and diarrhea (about 39%) were all far more frequent than on placebo. Most were mild to moderate and happened while the dose was being raised; about 3% of people stopped treatment because of side effects.
6.Does mazdutide help type 2 diabetes?
It is approved for type 2 diabetes in China, but GLORY-2 was an obesity trial — only about 16% of participants had diabetes — so it measured weight, not blood-sugar control. Weight loss was somewhat smaller in the participants who did have diabetes.
Sources
- Treatment With 9-mg Mazdutide for Weight Reduction in Chinese Adults With Obesity: The GLORY-2 Randomized Clinical Trial — JAMA (2026) · doi:10.1001/jama.2026.8142
- GLORY-2 trial registration (NCT06164873) — ClinicalTrials.gov
- Mazdutide and Orforglipron—New Evidence in Obesity and Diabetes (Editorial) — JAMA (2026) · doi:10.1001/jama.2026.10443
Not medical advice. Educational summary of published research. Last reviewed Jun 15, 2026.